 PREGNANCY
PREGNANCY  GIVING BIRTH
GIVING BIRTH  BABY CARE
BABY CARE  HEALTH & SAFETY
HEALTH & SAFETY  FUN STUFF
FUN STUFF  FAMILY
FAMILY Positions During Labor & Birth
[Adapted from The Birth Partner, by Penny Simkin. Copyright © 2008, used by permission of The Harvard Common Press.]
Position/Movement |
Unique Contributions |
|---|---|
Standing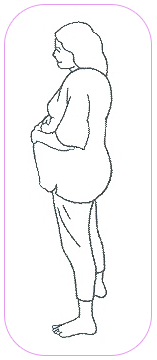 |
|
Walking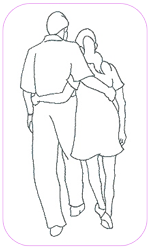 |
Same as standing, plus:
|
Standing and leaning forward on the partner, the bed, or a birth ball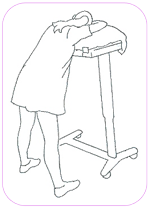 |
Same as standing, plus:
|
Slow-dancing:The mother leans against her partner, resting her head on his or her chest or shoulder. The partner's arms are under the mother's, around her back, with fingers interlocked at her lock back. She can tuck her thumbs into the partner's waistband or belt loops for comfort. They sway, perhaps to music, and breathe in rhythm. 
|
Same as standing, plus:
|
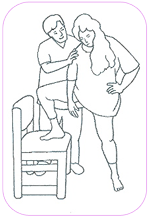
Standing lunge:Standing beside a chair and facing forward, the mother places one foot on the chair seat, with her raised knee and foot turned out. Bending her raised knee and hip, she "lunges" sideways repeatedly during a contraction (either in the direction that is more comfortable, or to the right for two or three contractions, and then to the left). She holds the stretch for two to five seconds at a time. She should feel the stretch in her inner thighs. Secure the chair, and help her keep her balance. |
|
Kneeling lunge:From starting position a, she bends her raised knee and hip and "lunges" sideways (as in b) repeatedly during a contraction in the direction that is more comfortable, or to the right for 2 or 3 contractions, then to the left for 2 or 3. She holds that stretch for 2 to 5 seconds at a time. She should feel the stretch in her inner thighs. |
Same as standing lunge 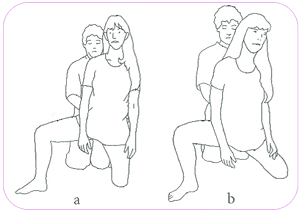
|
Sitting Upright
|
|
Sitting on a toilet or commode
|
Same as sitting upright, plus:
|
Semisitting
|
Same as sitting upright, plus:
|
Sitting and rocking in a chair or swaying on a birth ball
|
Same as sitting upright, plus:

|
Sitting, leaning forward with support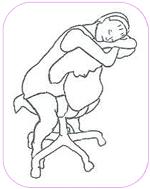
|
Same as sitting upright, plus:
|
Hands-and-knees position
|
|
Kneeling, leaning forward on a chair seat, the raised head of the bed, a birth ball, or the side of a tub
|
Same as hands and knees, plus:

|
Open knee-chest position:The mother gets on hands and knees, then lowers her chest, spreads her elbows, and rests her head on her hands. Make sure her knees are back far enough to raise her buttocks higher than her chest. You can support her by sitting on a chair, your feet about 9 inches apart. She puts her head between your shins, and leans her shoulders against them. 
|

|
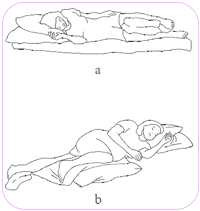
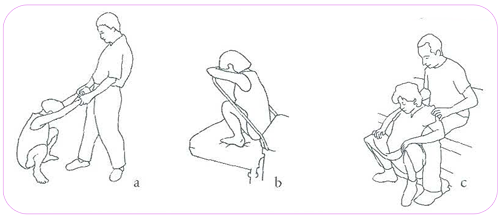
Side-lying or semiprone:In the side-lying position, the mother lies on her side with both knees flexed and a pillow between them (a). In the semiprone position, she straightens her lower leg, rolls slightly toward her front, flexes her top hip and knee, and rests the top knee on one or two pillows (b). During the birthing stage, you can hold the mother's top leg up as she pushes (c). 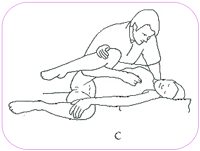
|
|
Squatting:The mother squats on the floor or bed, holding onto your hands (a), a railing, or a squatting bar (b) attached to the bed. Or, if you sit with your feet spread, she may stand between your knees (facing away from you) and lower herself into a squat, with her arms resting on your thighs for support (c). |
|
Lap Squatting:Sit on an armless straight chair. The mother sits on your lap facing you, straddling your thighs. Embrace each other. When a contraction begins, spread your thighs, allowing her buttocks to sag between. Have a support person or doula stand behind you and hold the mother's hands for safety. After the contraction, bring your legs together so the mother is sitting up on your thighs again. |
Same as squatting, plus:

|
Dangle with partner:Hold the mother under her arms as she leans with her back against you during contractions, and bear all her weight. Between contractions, she stands. |
Same as squatting, plus:
|
Dangle:Sit on the edge of a high bed or counter, with each foot supported on a chair and your thighs spread. Standing, the mother backs between your legs and places her flexed arms over your thighs. During contractions she lowers herself. Grip her chest with your thighs as she lowers. You support her full weight. Between contractions, she stands. |
Same as dangle with partner, plus:

|
On back with legs drawn up:The mother lies flat on her back and holds her knees apart and draws them to her shoulders. She lowers her legs between contractions. You can help her get into the position with each contraction. |
|
The Labor-Partner's Role
Here are the key functions of the labor partner:
- Be her advocate in communicating with the doctor, nurse-midwife and hospital staff.
- Call the doctor, nurse-midwife or hospital-staff when necessary.
- Be a calm, relaxing influence.
- Breathe with her. Learn the breathing techniques so you can help her with them.
- Use encouraging words such as: "You can do this!," and "I'm so proud of you!"
- Support her between contractions, reassuring her that she can do it!
- Bring her things to comfort her, like ice-chip, a cool washcloth, water, more pillows, a clean gown, etc...
- Keep yourself nourished, rested and comfortable: sit down now and then, eat, keep drinking water, take bathroom breaks.
Important Note: If you are helping her pushing efforts by helping her lift and hold her legs, be careful not to push her legs too far back.
Labor can be emotionally and physically challenging for you as a labor companion, but you are not having contractions and you are not in physical pain. Remember that there may be times when mother hits an emotional low, feeling that she cannot continue. She may be weeping. She may be so tense that she can't relax.
Your head is clearer and you have a better perspective. You can see that her despair is temporary and that she will pass through it. Here are steps you can take to help. You can "take charge."
- Be kind and calm, not panicked and loud.
- Put your face close to hers. Tell her to open her eyes and look at you.
- Walk her through the contraction. Breathe right along with her. Talk her through it.
- Be calm, confident and encouraging.
- Raise your voice slightly so that she pays attention and can hear you through her crying and her pain.
- Suggest a new position or a new way of handling the next contraction.
- Contractions and pain can make it difficult to concentrate. If she doesn't respond, tell her again, kindly and firmly.
- Continue to encourage her. Say things like "I know this is hard, and you're tired and it hurts. We only have to do one contraction at a time. We only have to get through this next one, OK? I'm right here, the nurse is here, and we're going to help you all we can. You're doing a great job!!" Remind her of your baby. It may help for her to remember why she is going through all of this.
Ask for Help
The doctor or nurse can help you by measuring dilation, suggesting new positions or a medical intervention that might help, and reassuring you and your partner that this is normal.
